MASKS
Some weeks ago we discussed here the use of masks and if they offered any level of protection.
At the time WHO was discouraging the use of masks outside medical professionals and saying the masks didn't offer any protection for common population.
Well that was just a big lie, the only reason for WHO to discourage the use of mask was to protect the existing stock of masks for Hospitals, and definitely there was a shortage and it would have been much bigger if everyone bought masks.
Now some countries, like mine, are preparing to remove progressively the lockdown measures so that economy starts rolling again.
One of the first measures is the Recommendation, and maybe soon mandatory, of the use of masks by everyone.
Government cites the examples of China and Macao (like other Asian countries), were the use of mask is enforced by law, as an example of the importance of the use of masks for protecting others and to protect yourself.
Well China and Macao were already an example of the use of masks 1 month and 2 months ago...
Wearing a mask properly, and this is important for it's efficiency, has to be learned.
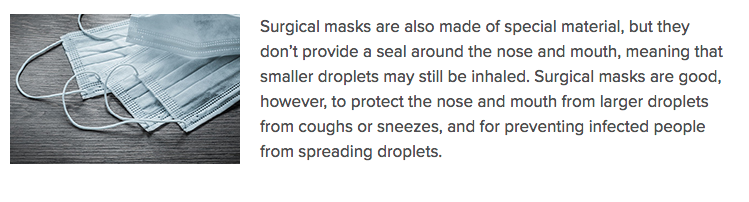
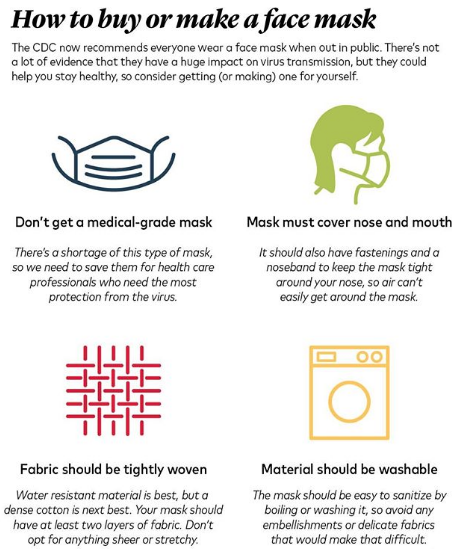
People have also to know what masks to use and not to use, for example simple surgical masks are the least effective.
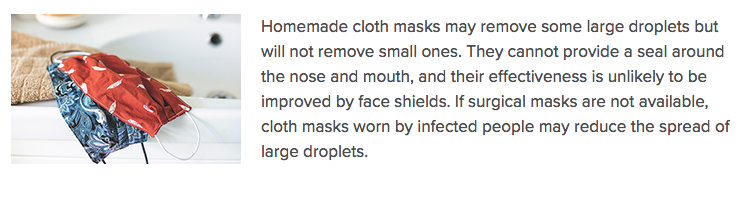
Making respirator masks at home or by cloths or textiles companies is possible.
It was clear to me since the beginning, and I wrote here before, that off course the use of masks by everyone would offer more protection than people not wearing it.
If everyone on a supermarket uses masks, you are protected by 2 masks, the mask you use but more importantly the mask other use, it's a double level of protection that will reduce by some small percentage your risk of getting infected. "Small" but impotant nonetheless.
So I would like to leave here somo information on masks that I think will be important for the next months, maybe year, were we will have to live with the virus around us:
Good video on the importance of using a mask and how to sew one:
https://www.youtube.com/watch?time_continue=119&v=q8GwjVihGj4&feature=emb_logo
How to Wear a Cloth Face Covering
1) fit snugly but comfortably against the side of the face
2) be secured with ties or ear loops
3) After fitting the mask don't touch it any longer. Just touch it to remove it at home by the ear loops
4) allow for breathing without restriction
include multiple layers of fabric, be able to be laundered and machine dried without damage or change to shape




")